Do I Need to Fill in Payer Name Continued
Guidelines for Filling HCFA Form
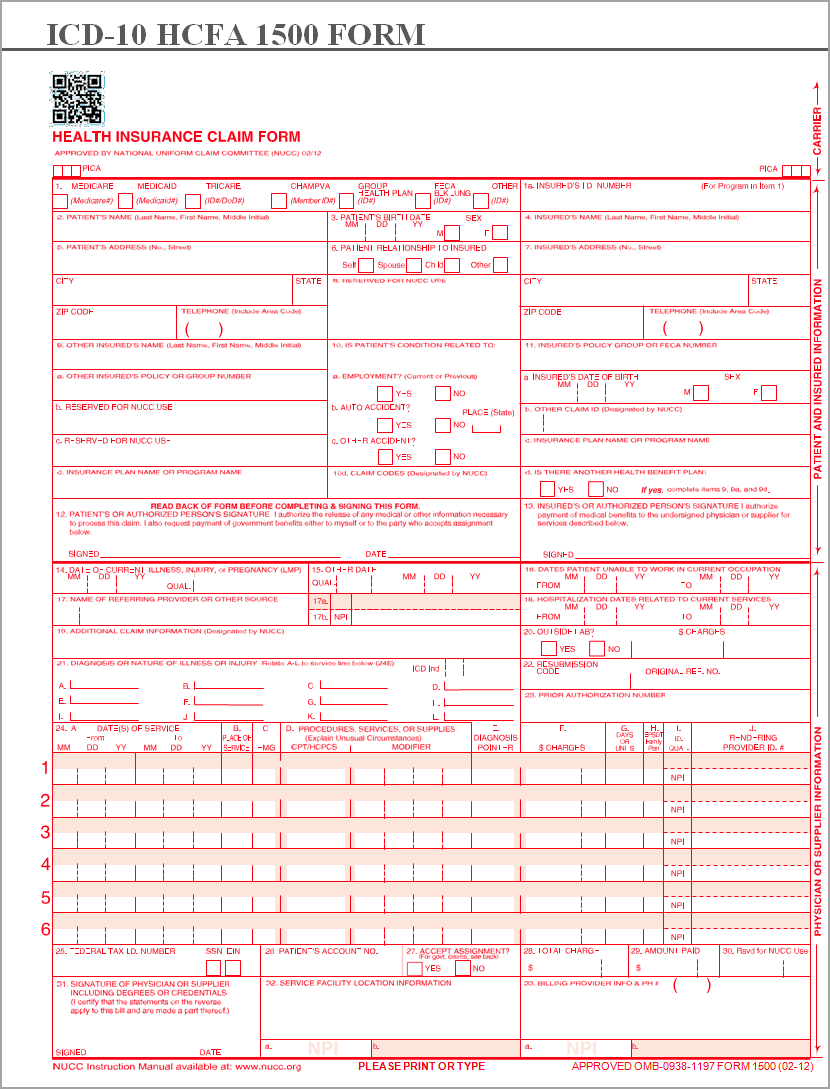
Table 1 explains each of the boxes in the HCFA Form
| Field # | Field Name | Field Description/Instructions |
| 1 | Coverage | PAYER TYPE of the destination payer. The type of health insurance coverage applicable to this claim by checking the appropriate box. |
| 1.a | Insured's ID Number | List the Insured's identification number entered in the subscriber# field of the destination payer in the Insurance Information screen under Patient Master. |
| 2 | Patient's Name | Patient's Last Name, First Name and Middle Name from the Patient Master. |
| 3 | Patient's Birth Date and Sex | Patient's Date Of Birth and Gender from Patient Master. |
| 4 | Insured's Name | Subscriber Last Name, First Name and Middle Name in the Subscriber Information section of the destination payer, in the Insurance Information screen under Patient Master. |
| 5 | Patient's Address | Patient's Address, City, State, Zip and Phone# from Patient Master. |
| 6 | Patient Relationship to Insured | Patient's Relationship to insured of destination payer in Insurance Information screen under Patient Master. |
| 7 | Insured's Address | Subscriber Address, City, State, Zip and Phone# in the Subscriber Information section of the destination payer, in the Insurance Information screen under Patient Master. |
| 8 | Reserved for NUCC Use | NA |
| 9 | Other Insured's Name | Subscriber Last Name, First Name and Middle Name in the Subscriber Information section of the Other payer, in the Insurance Information screen under Patient Master. [Section 9 is required only if Field 11d is marked "yes". if claim is for primary insurance other payer is secondary insurance, similarly if claim is for secondary insurance other payer is primary insurance and if claim is for tertiary insurance the other payer is secondary insurance] |
| 9.a | Other Insured's Policy or Group Number | Subscriber# of the other payer in the Insurance Information screen under Patient Master. |
| 9.b | Reserved for NUCC Use | NA |
| 9.c | Reserved for NUCC Use | NA |
| 9.d | Insurance Plan Name or Program Name | Other Insurance payer name from Insurance Information screen under Patient Master. |
| 10. | Is Patient's Condition Related to Employment/Auto Accident/Other Accident? | Information from the Accident tab in the Charge Entry or from the Accident section under Details tab in Charge Mater indicating the patient is treated for current or previous Employment/Automobile/Other accident. [State is required only if treated for Auto Accident] |
| 10.d | Claim Codes (Designated by NUCC) | Shows the value from Reserved For Local Use 10d field under Other tab as selected in Additional Information section under Charge Entry screen or as selected in the Details tab in encounter section under Charge Master screen. |
| 11 | Insured's Policy Group or FECA Number | Group# of the destination payer in the Insurance Information screen under Patient Master. |
| 11.a | Insured's Date Of Birth and Sex | Subscriber Date Of Birth and Gender in the Insurance Information screen under Patient Master |
| 11.b | Other Claim ID (Designated by NUCC) | Worker Comp. Claim# from Accident tab under Encounter section in Charge Master if provided; else blank |
| 11.c | Insurance Plan Name or Program Name | Destination payer name from Insurance Information screen under Patient Master. |
| 11.d | Is There Another Health Benefit Plan? | YESif there are multiple payers for the patient, and NO if there are no other payers for the patient. |
| 12 | Patient's or Authorized Person's Signature | Fills this information on selecting the option "Signed Signature Auth. or Claim Form for both Block 12 & 13 are on file" and enter the SIGNATURE DATE under Authorization Information section in Other Attributes page in Patient Master. |
| 13 | Insured's or Authorized Person's Signature | Fills this information on selecting the option "Signed Signature Auth. or Claim Form for both Block 12 & 13 are on file" under Authorization Information section in Other Attributes page in Patient Master. |
| 14 | Date of Current Illness, Injury or Pregnancy (LMP) and Qualifier | Shows first in the order Initial Treatment Date/Onset Date of Current Illness/Accident Date/Date of Pregnancy and the corresponding qualifier as selected in Additional Information section under Charge Entry screen or as selected in the details tab in encounter section under Charge Master screen. |
| 15 | Other Date | Shows first in the order Manifestation Date/ Accident Date/Last X-Ray Date and the corresponding qualifier as selected in Additional Information section under Charge Entry screen or as selected in the details tab in encounter section under Charge Master screen. |
| 16 | Dates Patient Unable to Work in Current Occupation | Shows the Date Patient Unable to Work From and To, as selected in Additional Information section under Charge Entry screen or as selected in the details tab in encounter section under Charge Master screen. |
| 17 | Name of Referring Provider or Other Source | Referring provider name as selected in the Charge Entry or Charge Master screens. |
| 17.a | Referring Physician ID | Provider Secondary ID and its Qualifier against the destination payer. State License Number (0B)/Provider UPIN Number (1G)/Provider Commercial Number (G2)/Location Number (LU) as setup in the Setup Secondary ID page in Provider Master. |
| 17.b | NPI | NPI of the Referring Provider shown in box 17 |
| 18 | Hospitalization Dates Related to Current Services | Shows the Admission Date From and To, as selected in Additional Information section under Charge Entry screen or as selected in the details tab in encounter section under Charge Master screen. |
| 19 | Additional Claim Information (Designated by NUCC) | Shows the value from Reserved For Local Use 19 field under Other tab as selected in Additional Information section under Charge Entry screen or as selected in the Details tab in encounter section under Charge Master screen. |
| 20 | Outside Lab? and Charge | Lab details entered in the Lab tab at Additional Information section in the Charge Entry or in the Lab tab under the Details tab in the encounter section under Charge Master. Mark as Yes in the HCFA form if outside lab box is selected and shows the amount entered in the Lab Charges field. |
| 21 | Diagnosis or Nature of Illness or Injury | Displays all the 12 Diagnosis selected in the Charge Entry or Charge Master with Diagnosis ICD 9/ICD 10 Indicator. |
| 22 | Resubmission Code and Original Ref. No. | Display corresponding codes for selected value from MEDICAID RESUB. CODE & MEDICAID ORIG. REF. CODE field under Encounter tab within Charge Master. |
| 23 | Prior Authorization Number | This field prints Authorization# or CLIA#: 1) If Authorization# exists, Authorization number corresponding to the Destination Payer selected in the Authorization# field in the Additional Information section under Charge Entry screen or in the details tab within encounter section under Charge Master Screen. 2) If Authorization# doesn't exists, CLIA# in Lab tab under Additional Information section under Charge Entry screen or that from the Details > Lab\Ambulance tab within encounter section under Charge Master Screen is shown. |
| 24.a | Date of Service | Encounter Date of Service entered in the Charge Entry or Charge Master. |
| 24.b | Place of Service | Encounter Place of Service selected in the Charge Entry or Charge Master. |
| 24.c | EMG | Displays Y if EMERGENCY check box is selected in Other tab within Additional Information section under Charge Entry screen or as selected in Others tab within the Details tab in encounter section under Charge Master screen. |
| 24.d | Procedures, Services or Supplies. | Lists the CPT codes selected in the encounter under Charge Entry or Charge Master and their corresponding modifiers if exists. |
| 24.e | Diagnosis Pointers | Lists the diagnosis codes against each CPT selected using corresponding diagnosis pointers as selected in the Charge Entry or Charge Master. |
| 24.f | Charges | Lists the Billed amount against each CPT as entered in the Charge Entry or Charge Master. |
| 24.g | Days or Units | Lists the Units entered against each CPT in the Charge Entry or Charge Master. |
| 24.h | EPSDT Family Plan | Displays Y if Family Plan check box is selected in Other tab within Additional Information section under Charge Entry screen or as selected in Others tab within the Details tab in encounter section under Charge Master screen. |
| 24.i | ID Qual. | Display 2 character SECONDARY ID TYPE Qualifier of the rendering provider against the destination payer entered in Setup Secondary ID page under Provider Master. |
| 24.j | Rendering Provider ID# | SECONDARY ID of the rendering provider against the destination payer entered in Setup Secondary ID page under Provider Master. [On the Top Colored area] |
| Shows the Rendering Provider NPI from the Provider Master. [On the bottom non colored area] | ||
| 25 | Federal Tax ID Number | Shows the Federal Tax ID or SSN according to the Rule below: 1) If the Rendering Provider Legal Entity is marked Account Separate YES and, a) If the Legal Entity Type is Non Solo, then populates the Federal Tax ID from the Legal Entity of Rendering Provider. b) If the Legal Entity Type is Solo, then populates the Federal Tax ID of the Rendering Provider. 2) If the Rendering Provider Legal Entity is marked Account Separate NO and, a) If the Entity Type of Primary Legal Entity is Solo, then populates the Federal Tax ID of the Rendering Provider. b) If the Entity Type of Primary Legal Entity is Non Solo, then populates the Federal Tax ID from the Primary Legal Entity. |
| 26 | Patient's Account Number | Shows the Claim# after claim generation. |
| 27 | Accept Assignment? | Displays Yes/No according to the selection of Medicare Participating from Provider Master. |
| 28 | Total Charge | Total Charge in this claim. i.e. sum of all charge in box 24.f |
| 29 | Amount Paid | Total Amount Paid for this encounter by the patient and other payers against the services billed. |
| 30 | Reserved for NUCC Use | NA |
| 31 | Signature of Physician or Supplier Including Degrees or Credentials | Shows the Rendering Provider Name and Credentials along with the Signature on File and Claim Date. |
| 32 | Service Facility Location Information | Shows the details like Name, Address, City, State and Zip of Services Location that selected in the Charge Entry or Charge Master. |
| 32.a | NPI | Shows NPI of the Service Location that selected in the Charge Entry or Charge Master. |
| 32.b | Other ID | Blank |
| 33 | Billing Provider Info. and Phone# | Populates the data according to the Rule below: 1) If the Rendering Provider Legal Entity is marked Account Separate YES and, a) If the Legal Entity Type is Non Solo, then populates the Name and Payable to address of the Rendering Provider Legal Entity. b) If the Legal Entity Type is Solo, then populates Name and Address of the Rendering Provider. 2) If the Rendering Provider Legal Entity is marked Account Separate NO and, a) If the Entity Type of Primary Legal Entity is Solo, then populates Name and Address of the Rendering Provider. b) If the Entity Type of Primary Legal Entity is Non Solo, then populates the Name and Payable to address of the Primary Legal Entity. |
| 33.a | NPI | Populates the data according to the Rule below: 1) If the Rendering Provider Legal Entity is marked Account Separate YES and, a) If the Legal Entity Type is Non Solo, then populates the Group NPI of the Rendering Provider Legal Entity. b) If the Legal Entity Type is Solo, then populates NPI of the Rendering Provider. 2) If the Rendering Provider Legal Entity is marked Account Separate NO and, a) If the Entity Type of Primary Legal Entity is Solo, then populates NPI of the Rendering Provider. b) If the Entity Type of Primary Legal Entity is Non Solo, then populates the Group NPI of the Primary Legal Entity. |
| 33.b | Other ID | Displays 2 character SECONDARY ID TYPE Qualifier & SECONDARY ID for the rendering provider against the destination payer entered in Setup Secondary ID page under Provider Master. |
Table 1
Source: https://academy.practicesuite.com/guidelines-for-filling-hcfa-form/
0 Response to "Do I Need to Fill in Payer Name Continued"
Post a Comment